Signed in as:
filler@godaddy.com

Bartholin cysts and abscesses are some of the most common gynaecological problems, accounting for 2% of all gynaecological presentations to the hospital. The traditional treatment is marsupialisation, which requires a general anaesthetic and is associated with significant post-operative pain. Thanks to surgical advances, these can now be effectively treated using only local anaesthetics with the insertion of a Word catheter.
An ectopic pregnancy is one that has implanted outside the uterine cavity and affects ~2% of all pregnancies. The most common site for an ectopic pregnancy is in the fallopian tube and if surgical management is warranted, most gynaecologists remove the fallopian tube involved. However, in many cases minimally invasive, fallopian tube-preserving surgery in the form of laparoscopic salpingotomy is feasible.
This is a rare pregnancy that has implanted at the site of a previous Caesarean section scar. This is an extremely high-risk pregnancy that in very select cases are allowed to continue and sometimes result in a live birth. In most cases, treatment with intra-sac and systemic methotrexate is recommended. However, due to the prolonged admission associated with methotrexate treatment, surgical management by an expert gynaecologist should be considered.
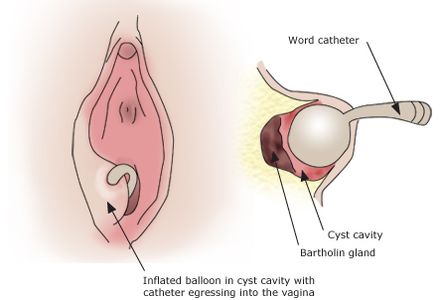
Bartholin cysts and abscesses, which are traditionally treated by marsupialisation under general anaesthesia, can now be effectively treated using only local anaesthetics with the insertion of a Word catheter.
According to the WoMan-Trial published by Dutch gynaecologist Dr Kroese in the British Journal of Obstetrics and Gynaecology in 2016, compared to marsupialisation, insertion of a Word catheter for the treatment of Bartholin cysts and abscesses:
1. Does not require a general anaesthetics and therefore does not require pre-anaesthetic fasting or a prolonged wait to be operated on;
2. Is just as effective with similarly low rates of recurrence;
3. Is associated with less post-procedural pain and therefore patients required less pain relief.
The findings were so overwhelmingly positive, Dr Stephen Lee introduced the treatment modality to the Royal Women's Hospital to successful outcomes and positive patient feedback.

Determining the best treatment for a Caesarean scar pregnancy is a complicated process. One of the predictors for the success rate of medical management with methotrexate is a scoring system devised by Dr Dior's team and published in the Journal of Minimally Invasive Gynaecology in 2019. This scoring system takes into account the pregnancy's gestational age, beta-HCG levels, gestational sac size and the absence or presence of abdominal pain.
In many cases, treatment with intra-sac and systemic methotrexate is recommended. However, due to the prolonged admission associated with methotrexate treatment, surgical management by an expert gynaecologist should be considered. Particularly if the Caesarean scar pregnancy is classified as type 1, which means the gestational sac is developing towards the endometrial cavity, surgical management can sometimes be a straightforward suction curettage. With a type 2 Caesarean scar pregnancy on the other hand (see picture above), laparoscopic removal of the Caesarean scar pregnancy by an experienced set of hands is required. One advantage of the laparoscopic approach is that the Caesarean scar defect can be excised and repairs at the same time.